Clinical case: Triad in a European cat

Patrick LECOINDRE
Docteur Vétérinaire

ANAMNESIS
A 7 year old, 3.2 kg, neutered female European cat, is presented with persistent chronic profuse diarrhea over the past two months. A weight loss of 500 g is reported despite a retained appetite. During the last two weeks, the cat was lethargic and dysorexic.
CLINICAL INVESTIGATION
On clinical examination the cat is weak but still reactive. The body condition score is assessed at 2/6. The abdominal palpation is flexible and painless, however the intestinal loops are thickened. No thyroid nodules have been palpated. 8% dehydration is estimated. Mucous membranes appear icteric. The remainder of the clinical examination was without abnormality.
DIAGNOSTIC HYPOTHESES
Chronic diarrhea associated with weight loss despite normal food intake leads to malassimilation/malabsorption. Chronic diarrhea can have two main origins. A digestive origin with chronic inflammatory bowel disease and low grade intestinal lymphoma are to be evoked in priority. Among the extra digestive causes, diseases of the bile ducts, cholangitis, pancreatitis, hyperthyroidism, renal insufficiency are to be considered. Jaundice can be of pre-hepatic, hepatic or post-hepatic origin.
FURTHER EXAMS
The blood count reveals a moderate normochromic normocytic anemia suspected primarily of an inflammatory component (Ht=16.8%, Hb=5.6 g/dL, GR=2.28 M/μL, indices in the usual values). A non-specific neutrophilic leukocytosis (GB=22.1 M/mL of which PNN=19.4 M/mL) is present. These tests allow us to rule out a prehepatic origin of jaundice.
The biochemical analysis shows a major elevation in the parameters of hepatic cytolysis and cholestasis (PAL=520 U/L, ALAT=545 U/L, GGT=45UI/L, Bili=96.4 mg/L). Discrete hypokalemia at 3.4mmol/L is present. It should be noted that in cats, GGT has some specificity for cholangitis. The Snap fPL is positive with a SpecfPL assay at 8.9 μg/l (VU < 3.5). Hypocobalaminemia is noted at 220 pg/ml (UV > 900).
An ultrasound examination of the abdomen was performed. Hepatic parenchyma appears discreetly hyperechoic. The gallbladder is slightly distended with no visualized obstructive signs. It presents a thickened wall with heterogeneous contents. The pancreas is abnormally visible, enlarged and echogenic. There is a slight mesenteric adenomegaly. Both pancreatic lobes show a very moderately heterogeneous echostructure. Diffuse, regular and moderate thickening of the walls of the small intestine is also noted.
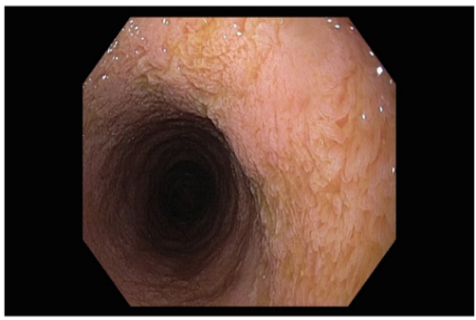
An endoscopy showed an abnormally granular duodenal mucosa. Staged biopsies are taken.
DIAGNOSTIC HYPOTHESES
Faced with a rough symptomatology that associates anorexia and despondency, intermittent digestive signs, signs of cholestasis, the diagnosis is in favour of a complex triad, a chronic inflammatory bowel disease, acute or chronic pancreatitis, probably neutrophilic cholangitis with cholecystitis.
A definitive diagnosis of triad is based on histopathological evaluation of each organ.
Liver biopsies are performed under laparoscopy. Similarly, cholecystocentesis is performed in order to carry out a bacteriological examination of the bile as well as a cytological analysis. The contents are very thick and modified, the bacteriology reveals an E. coli sensitive to all the antibiotics tested. The cytological analysis confirms the presence of numerous degenerated neutrophils with bacilli in intracellular position. Hepatic histology reveals neutrophil ranges in the periportal zone, around the bile ducts. Histological examination of digestive biopsies reveals moderate grade lymphoplasmacytic enteritis.
DIAGNOSIS
The presence of concomitant pancreatic and hepatic intestinal inflammation points to a diagnosis of feline triad.
MANAGEMENT
The insertion of an esophagostomy tube allows the initiation of a supportive enteral feeding plan. Post-operative management combines antibiotic therapy (amoxicillin 20 mg/kg SC BID - metronidazole 15mg/kg PO BID) and corticosteroid therapy (prednisolone 1 mg/kg IV BID) which is initiated due to intestinal inflammation. The remainder of the therapeutic plan consists of an antacid (ranitidine 2mg/kg IV BID), an anti-vomitant (maropite citrate 1 mg/kg IV SID), a choleretic (ursodeoxycholic acid 10 mg/kg/PO SID), L-carnitine 30-50 mg/kg in the maintenance infusion (LR at 2 ml/kg/h with potassium supplementation according to the monitoring of kalemia). Vitamin K treatment is performed
before the laparotomy. This is based on the high prevalence of vitamin K-sensitive coagulopathies in cats with intestinal disease and hepatobiliary. Maropitant (NK1 receptor antagonist) at 1mg/kg is very useful for controlling nausea. It also seems that this molecule has an effect visceral analgesic.
EVOLUTION
There is a progressive improvement in the cat's general condition during the hospitalization with a recovery of appetite after 3 days. At D+6, bilirubinemia is 7.4 mg/L, Spec fPL of 4.1 μg/L and GGT of 11 IU/L. The animal is returned after 8 days of hospitalization, with treatment combining ursodeoxycholic acid (15mg/kg/day), metronidazole-based antibiotic therapy (15mg/kg BID) for 6 weeks, corticosteroid therapy (1 mg/kg/day at decreasing doses up to a dose of 0.5mg/kg every 2 days over 2 months). An injection of vit B12 at 250μg is recommended once a week for 5 weeks.
COMMENTS
« Triad » is the term used to describe the concomitant inflammation of the pancreas, liver and small intestine. Triaditis has been reported in 50-56% of cats with pancreatitis and 32-50% of those with cholangitis/inflammatory liver disease. A definitive diagnosis of triaditis is based on histopathological evaluation of each organ. Treatment requires antibiotic therapy on several weeks.